AMA: The Strongest Trade Union in the U.S.A.

As a follow-up to the post below on Milton Friedman's Mayo Clinic talk on the "economics of medical care," I present the two charts above.
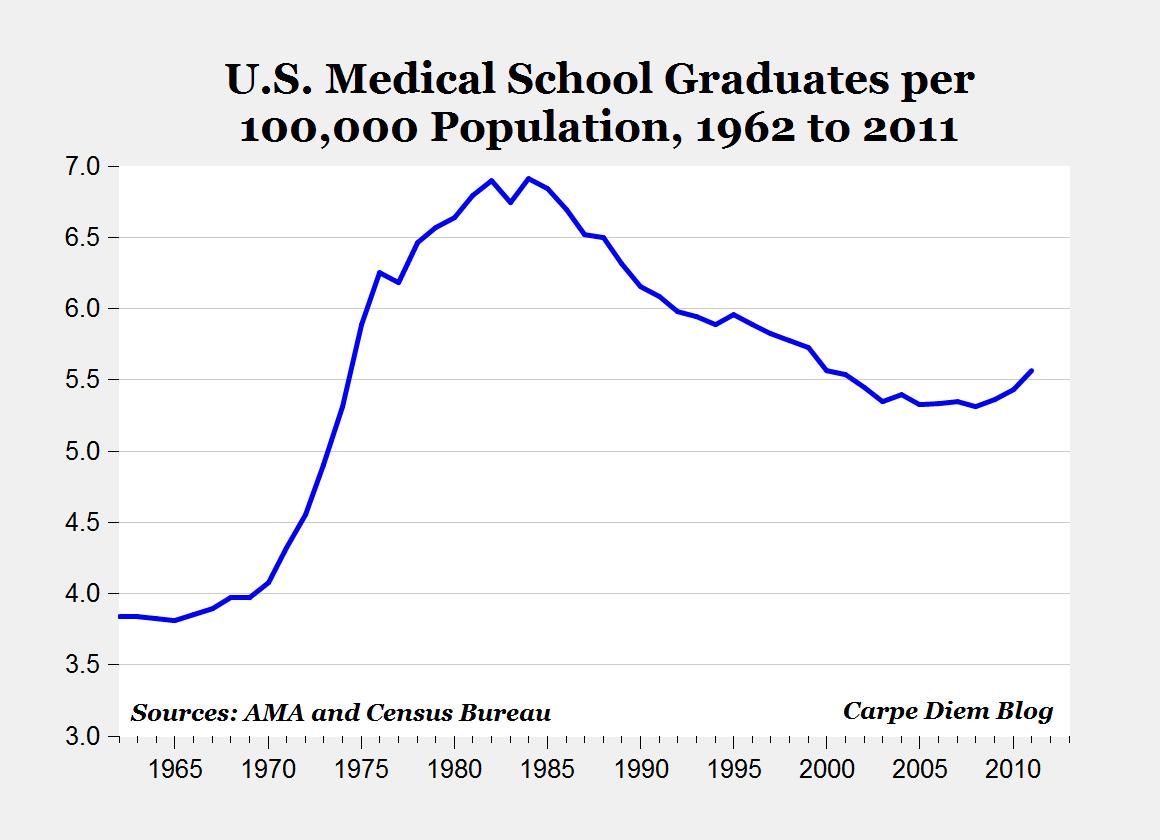
The top chart shows the number of annual graduates from U.S. medical schools (AMA data here) per 100,000 U.S. population, from 1962 to 2011. Between about 1970 and 1984, there was a significant increase in medical school graduates that pushed the number of new physicians from 4 per 100,000 Americans in 1970 to almost 7 per 100,000 by 1984. Since 1984, the number of medical school graduates has been relatively flat (see red line in bottom chart), while the population has continued to grow, causing the number of new physicians per 100,000 population to decline to only 5.3 per 100,000 by 2008, the same ratio as back in 1974. Over the last few years the number of medical school graduates has increased slightly, and the ratio of graduates per 100,000 increased to 5.56 last year, the highest in a decade.
The bottom chart compares the actual number of medical school graduates (red line) to the projected number of graduates if the number of new physicians had keep pace with U.S. population increases, i.e. the ratio of graduates per 100,000 Americans had stayed at the 1984 level of 6.91. In that case, we would now be graduating close to 22,000 new doctors annually, and the cumulative increase in medical school graduates from a rate of 6.91 per 100,000 population over the last 27 years would mean that we would have 84,000 additional physicians today.
In most professions, as the population grows and the demand for those occupations increase, we would expect to see an increase in the number of people employed in those professions. Over the last 25 years, the U.S. population has both increased in size, and gotten significantly older on average due to increasing life expectancy, and both of those factors would put upward pressure on the demand for physicians. But in the case of medicine, the supply of students entering medical schools has been restricted relative to the growing population, leading to an insufficient supply of doctors, and higher-than-market wages. This restriction on the supply of doctors relative to a growing population is one example of the "power of organized medicine" that Milton Friedman talks about in his lecture at the Mayo Clinic.
Also, in his classic 1962 book Capitalism and Freedom, Dr. Friedman describes the American Medical Association (AMA) as the "strongest trade union in the United States" and documents the ways in which the AMA vigorously restricts competition. For example, the "Council on Medical Education and Hospitals" of the AMA approves both medical schools and hospitals. By restricting the number of approved medical schools and the number of applicants to those schools, the AMA effectively limits the supply of physicians, which increases their wages, and raises the overall cost of medical care.

157 Comments:
The President says that Obamacare will bring at least 10 million more people into the healthcare system. Maybe they will be seen by the 16,000 new IRS agents?
Family physicians are decreasing dramatically in the U.S. In looking for a chart on general practioneers on Bing I found a great Carpe Diem blog post and chart on this subject (scroll down).
Note the the last comment, which is quite smug but not prophetic.
doctors are also gatekeepers to healthcare products and services. A low number of doctors creates a bottleneck in access to these products and services, which inflates prices.
These medical schools don't expand to meet demand either. If they acted like for-profit businesses, they'd be 100 times as large and have surplus seats available, and they'd make a lot more money, too. Instead they rarely if ever grow enrollment year over year, nor do they build new campuses in areas where there is demand. They prefer to be ever more selective, and raise the price of tuition every year.
" A low number of doctors creates a bottleneck in access to these products and services, which inflates prices"...
It just might get lower now...
From the DOCTOR PATIENT MEDICAL ASSOCIATION FOUNDATION survey dated June, 2012
KEY FINDINGS
90% say the medical system is on the WRONG TRACK
83% say they are thinking about QUITTING
61% say the system challenges their ETHICS
85% say the patient-physician relationship is in a TAILSPIN
65% say GOVERNMENT INVOLVEMENT is most to blame for current problems
72% say individual insurance mandate will NOT result in improved access care
49% say they will STOP accepting Medicaid patients
74% say they will STOP ACCEPTING Medicare patients, or leave Medicare completely
52% say they would rather treat some Medicaid/Medicare patient for FREE
57% give the AMA a FAILING GRADE representing them
1 out of 3 doctors is HESITANT to voice their opinion
2 out of 3 say they are JUST SQUEAKING BY OR IN THE RED financially
95% say private practice is losing out to CORPORATE MEDICINE
80% say DOCTORS/MEDICAL PROFESSIONALS are most likely to help solve things
70% say REDUCING GOVERNMENT would be single best fix.
Isn't the bottleneck after med school in internships and residencies?
Dentists have been even more successful at blocking entry into the profession, and dentists now have higher average incomes than physicians.
If you go to the below link to AMA data you will find the number of Medical School grads in 2011 is remarkably higher relative to previous years. Appox 1,200 MORE than in 2007. The numbers are static going back 20 years, as D Perry has noted. So, they do have the power to increase the number of doctors pretty quickly, IF they want to.
https://www.aamc.org/download/145438/data/table27-grad-0711.pdf
It is suggested the graph showing medical school graduates peaking in the 1980 - 90 period more probably reflects the post-WW2 baby boomers moving through all professional schools.
This tirade against the AMA would have somewhat more credibility if your graph were normalized for that effect.
All statistical trends and fluctuations are not caused by evil conspiracies of professional associations.
This tirade against the AMA would have somewhat more credibility if your graph were normalized for that effect.
That's what the second graph shows.
"That's what the second graph shows."
No it doesn't. The second graph shows the pre-1970 trend repositioned and extended from the peak in about 1985.
The second graph shows projected med school graduates based on the growth of population both projected (based on previous rates) and actual. That should account for the Baby Boomers.
If you like our agriculture sector, if you like the Defense Department, then you are going to love Obamacare.
Importing foreign Doctors is a no-brainer...
Yet the cartel blocks this..
On a work-hours equivalent basis, the numbers are worse than appear in your chart.
On November 24, 2009, you published on this blog a chart of medical school graduates by gender. In 1980, about 25 percent of the graduates were women, in 1985, 30 percent and currently about 50 percent are women.
Other studies have found women doctors on average work fewer hours than male doctors, take maternity leave and time off to raise children (though of shorter duration than in other jobs) and tend to concentrate in a few specialties, such as pediatrics.
The number of doctor-hours available as GPs, or in specialties outside of pediatrics and the few others chosen by women, is much more below population trend and worse than your chart indicates.
I also note that if Obamacare does in fact make Doctor salaries go down even 20%, immigration of Doctors will greatly reduce..
Doctors (and Dentists) are the only profession in which the US wage is over twice as much as Canada or Europe.
The effect this has had on immigration of Doctors to the US should not be understated, nor is the effect of this inflow stopping.
"We were surprised to learn this month from the Canadian Medical Association Journal (CMAJ) the extent of the doctor drain to the United States. One in nine Canadian-trained doctors -- including one in five specialists -- is now practicing in the United States. We suspected the number was high, but not that high. No wonder there is a shortage of doctors in Canada, and nearly two million of us are without a family physician.
It's also not hard to see the underlying cause of the exodus: socialized medicine. The exodus began in the mid-1980s, coinciding with the passage of the Canada Health Act (CHA), which all but outlawed private care, forbade user fees and banned extra billing by physicians. Fed up with government-monopoly health care, many voted with their feet. The CMAJ authors (Robert L. Phillips, Jr., Stephen Petterson, George E. Fryer, Jr. and Walter Rosser) conclude that about 12,000 Canadian-educated physicians are now living in the United States.
As the authors point out, "this is the equivalent of having two average-sized Canadian medical schools [out of a total of just 17] dedicated to producing physicians for the United States," every year for 25 years." -- Canada.com
It would be one thing if the supply and demand of doctors determined the price a doctor can charge. Even with a supposed shortage of doctors, their salaries have been going down on a yearly basis due to medicare cuts and regular insurance making similar percentage-wise cuts. IOW, the control of the number of doctors has no determination on the cost of medical care from these physicians.
It would be one thing if the supply and demand of doctors determined the price a doctor can charge. Even with a supposed shortage of doctors, their salaries have been going down on a yearly basis due to medicare cuts and regular insurance making similar percentage-wise cuts. IOW, the control of the number of doctors has no determination on the cost of medical care from these physicians.
Malpractice attorneys driving doctors away?:
Cost of malpractice insurance forcing doctors to leave high-risk specialties
March 13, 2008
"In New Hampshire, many physicians are leaving as malpractice insurance costs soar.
Specialty physicians have experienced a 50 percent increase in premiums from five years ago. The average premium is now close to $100,000 for obstetricians and neurosurgeons.
The U.S. Department of Health and Human Services has estimated medical liability costs add $60 billion to $108 billion to the cost of health care each year.
Interestingly, the estimated annual cost of covering all of the uninsured patients in the United States is $100 billion."
Also, "defensive medicine" adds to medical liability costs.
"Malpractice has both direct and indirect costs, including "defensive medicine." According to the American Medical Association, defensive medicine increases health systems costs by between $84 and $151 billion each year."
I have often wondered what effect Pharmaceutical direct advertising has had on doctors. Are doctors just order takers now? Seems they have been marginalized.
Wow, everyone is in basic agreement!
Cool.
re: tort costs
" According to the actuarial consulting firm Towers Perrin, medical malpractice tort costs were $30.4 billion in 2007, the last year for which data are available. We have a more than a $2 trillion health care system. That puts litigation costs and malpractice insurance at 1 to 1.5 percent of total medical costs. "
PeakT's numbers are a bit higher but again when that number is compared to the total health care system, it appears to be in the low percent range not a major cost driver.
re: shortage of doctors
US doctors make, on average, twice as much as most other country's doctors.
I'm not sure how foreign doctors are stopped from coming here but the interesting thing locally is that we're seeing more and more foreign surnames for things like endocrinology and oral surgeons.
Not only foreign surnames but personal experience thick accents ... and the office staff speak the same native country language as the doctor which is a bit disconcerting when in front of you they start speaking in their native language in discussing you!
so a gentle provocative question:
does the increase in the need for doctors and planned increase in IRS agents mean that ObamaCare CREATES jobs?
:-)
So is the problem that doctors are paid too much (Milton Friedman, Dr. Perry) or that doctors are paid too little (kmg, Cindy Martin)??
Or maybe it is both at the same time?? Doctors think they are paid too little; and those who pay the bills think doctors are paid too much.
well it's not just what the Doctor makes - it's the prices the doctor has to charge to cover all his expenses including his office staff and rent.
We're seeing doctors locally abandoning high rent office space and moving to more modest digs.
But I also observe this at my Primary Care doctor and that is she appears to have an office staff of 10-15 and most all of them dealing with paper records... faxing stuff...etc....
I think the Feds are actually offering grants now for Doctors to move to electronic systems.
What I'd find interesting is a cost breakdown of a doctor's bill to see how much goes to him and how much goes to other costs.
Right now, I'm not at all sure when I pay the doctor bill - how much the doctor actually gets to keep out of the total bill but I'm betting less than half or perhaps even less.
so the costs for health care involve MORE than just doctor salaries and in countries where there are electronic records where you can go to any doctor who can then pull up your entire medical history on a computer screen, it's got to be cheaper.
Imagine if, in this country, you could go to a doc-in-the-box and they could instantly pull up your medical history electronically (with your permission)...
it would save you time and money and you'd get a more precise diagnosis and likely a more precise course of treatment.
Note too that most doctors do not want to remain GP's. The cost of medical school is high in terms of money and time. GPs earn relatively little. Doctors prefer specialties where they earn more.
Also interesting is how many surgeons prefer to perform plastic surgery (cosmetic dentistry in the case of dentists - which may in part explain higher incomes. I don't know). Cosmetic surgery is not covered by insurance, yet doctors become very wealthy in that area of medicine.
It's interesting that people of even modest means find the cash to pay for plastic boobs and rhinoplasty but become incensed when they have to pay to get their appendix removed.
Obamacare provides strong incentive to avoid becoming an overworked general practitioner (just the guy you want on the front line of your medical issues, eh?) and go into a specialty.
From the Census link below---Since 1980 the average yearly NET change (new entrants minus exiters) in MD's with US medical school degrees is 12,068. The average net change in MD's for foreign medical school degress is 5,310. Total average change in 29 years of 17,378 per year--domestic plus "foreign". If we are "importing" 30% of our physicians, seems like there is room for improvement domestically. It might be even worse---the data notes that the total number of MD's include a relatively large number of doctors that are "inactive or address not found"
https://docs.google.com/spreadsheet/ccc?key=0AtrXvCHP3uxcdDltWkw2Q1gzV0UwWURpY3hYWTlCTmc#gid=0
re: going to a specialty over GP.
that's been happening for a decade or more long before anyone knew about "ObamaCare".
The health care system we have right now - the private health care system will pay for expensive procedures by specialists and Doctors like others will move to the areas that are more lucrative.
Medicare and MedicAid are much tougher on what they pay for and Medicare requires a 20% co-pay unless someone has purchased Medicare Advantage to cover the 20%.
But even then, there are some things that Medicare will not cover - at all - including most dental and glasses. (not sure about Lasik, etc).
A good question is perhaps does Medicare and MedicAid encourage GPs moving to specialty practices?
Yeah, Ed R. Professional associations usually want what's best for the customer, not its members.
For instance, members of a professional association in my profession recently lobbied the SEC to forcibly create wider markets in illiquid stocks in order to increase the profit margin to attract more market makers. Of course, the whole rationale for market makers is that they compete with each other to narrow the bid/ask spread for customers.
There's nothing I love more than the government selling to the public a story about creating a group of protected insiders in order to lower costs for them only to erase that benefit, forcing my customers to pay more for my product. Let the undeserved profits tumble into my pocket from yours! Thank the Lord for fools who look to licensing and regulation to protect them....against lower prices and better service.
that's been happening for a decade or more long before anyone knew about "ObamaCare".
Yes, dippy. That started with the other great government programs - medicare and medicaid. Obamacare will make that significantly worse.
I don't really know how many times it has been pointed out to you that Lasik is never covered by any insurance (that's why the price has tanked while technology and outcomes have improved). I've said it a few times just in the the past couple of days. Paul has mentioned it. And yet, you're still not sure if Lasik is covered.
sorry I missed that part ...
but Medicare and MedicAid do not cover quite a bit, and require a significant co-pay even if they do and what they actually cover is usually quite a bit less than the charged fee.
We even have people saying HERE that Medicare reimbursements are SO LOW that doctors are starting to REFUSE new Medicare and MedicAid patients.
So you arguing both sides here - that one one hand that Medicare/MedicAid drives up costs and on the other hand it's reducing the number of Drs who will take Medicare/MedicAid.
so which is it?
so the costs for health care involve MORE than just doctor salaries and in countries where there are electronic records where you can go to any doctor who can then pull up your entire medical history on a computer screen, it's got to be cheaper.
Another great myth that refuses to go away. If electronic record keeping is such a great idea and so efficient, why are admin staffs continuing to grow like Iowa corn? Show us one bureaucracy that has shrunk in response to digital filing.
Ed R: "the graph showing medical school graduates peaking in the 1980 - 90 period more probably reflects the post-WW2 baby boomers moving through all professional schools."
I was going to use real data to refute this assertion by Ed R, and then discovered Ed R may be correct.
The typical physician will complete medical school about age 26. Let's assume for a moment that the number of foreigners in U.S. medical schools hasn't varied significantly. If so, then the number of medical school graduates should mirror live births with a lag of 26 years.
Here's U.S. live births (millions)
1950___3.5
1955___4.1
1960___4.3
1965___3.8
1970___3.7
1975___3.1
1980___3.6
1985___3.8
Here's medical school graduates
(thousands)
1976___13.8
1981___15.3
1986___16.0
1991___15.4
1996___15.9
2001___15.8
2006___15.9
2011___17.4
Note: I don't have the actual data for graduates for every year, so I estimated the number using Prof Perry's graph.
IMO, it is remarkable that medical school graduates stayed above 15,000 per year in the 1990s. That's when the children from the baby bust years were graduating from medical schools. Foreign students are part of the answer. The liberation of women to pursue work in previously male-dominated fields is another.
As I understand it, medical schools desire to maintain very high intelligence levels for admissions. At the same time that the global 1970s baby bust caused a reduction in availability of high IQs, other career opportunities for highly intelligent persons were also soaking up the potential medical school graduates.
I'm not convinced the strength of the AMA was the major reason for the supply of MDs not keeping up with the demand. Of course, the AMA has been successful in limiting the spread of alternate services (Nurse Practitioners, for example.)
so which is it?
Both. The two are not mutually exclusive.
M & M causes costs to rise as more and more people become part of the system. The demand for services rise, causing prices to rise. Since patients do not bare the full cost of these services, they have no issue requesting tests and the like that they may not need. Costs rise.
Likewise, reimbursements fall, either in nominal amounts, or they do not rise fast enough to keep up with the costs of care. So, doctors are being charged more and more for these services but receive less and less in reimbursements.
"" A low number of doctors creates a bottleneck in access to these products and services, which inflates prices"."
there is no bottleneck of doctors.
there is a bottleneck of doctors willing to be gouged by medicare/aid. few will take new patients because they lose money every time they see one.
if you have good private insurance, there is little issue getting in to see any kid of doctor. if you pay cash, there is no issue at all.
this is not a supply problem so much as it a problem with artificially high levels of demand from specific sectors.
this is a great video on this from the prolific and excellent OMID:
http://youtu.be/I7pqRjHQ9BU
but Medicare and MedicAid do not cover quite a bit, and require a significant co-pay even if they do and what they actually cover is usually quite a bit less than the charged fee.
That's right, Larry. You are now face to face with the defining characteristic of government-run programs (not just THIS government's programs, mind): You pay more to get less.
Where there is competition and government and third party payers are NOT involved, you continue to get more for less.
The poor once couldn't afford dishwashers, air conditioning, telephones, cell phones, new clothing, etc. Now, all of those things are ubiquitous. Why? There is significant incentive for providers of those things to reduce the price as much as possible. The bigger their market, the more people can afford their services or products, the more money they can make and the more stable their business is because they are not dependent on a niche market.
That is why a competitive market is better for that little boy in your previous example. There is every incentive for providers to compete with each other to attract patients. And that is also why Singapore's universal health care is superior. While the government shells out a certain amount, providers must compete with each other for those health care dollars.
if you pay cash, there is no issue at all.
And that is why I pay cash. Most of my doctors refuse to deal with insurance at all.
But, the graphs do point to a supply problem. As the population grows, the number of med school graduates declines. There is a shortage of physicians in geriatric medicine. There is a shortage of GPs. There is a shortage of pediatric dentists, etc. All of these are typically reimbursed by a third party payer. There is NO shortage of plastic surgeons. They are paid directly by the patient.
As I understand it, medical schools desire to maintain very high intelligence levels for admissions.
I remind you that George Balella (Muirdiot) is a med school graduate. My cousins would avoid at almost any cost about half of their med school classmates and let's not forget lower standards if you happen to belong to certain politically favoured groups.
At the same time that the global 1970s baby bust caused a reduction in availability of high IQs.
Why would that be? IQ's are genetically determined . As a percentage of new births, they should have remained about the same. If being a doctor is so rewarding, wouldn't you expect at least the same percentage of the population to opt for medical school? UNLESS patients can now see non-doctors for some of their care. But, there's no significant movement on that front because the AMA chokes that off.
other career opportunities for highly intelligent persons were also soaking up the potential medical school graduates.
Perhaps that explains Muirdiot. Med schools were left with dregs. Of course, part of the reason may be artificially high costs of going to medical school resulting from the AMA's choke hold on the profession. The pay-off for graduating medical school is not as high as graduating business school or even maybe law school - the two other professions potential doctors usually consider.
"It's interesting that people of even modest means find the cash to pay for plastic boobs and rhinoplasty but become incensed when they have to pay to get their appendix removed." -- Methinks
Simultaneously, the funniest and most insightful thing posted on this comment thread.
methinks: "Why would that be? IQ's are genetically determined . As a percentage of new births, they should have remained about the same. If being a doctor is so rewarding, wouldn't you expect at least the same percentage of the population to opt for medical school?"
Did you notice the part of my comment about the 26 year lag between birth of a potential doctor and his graduation from medical school?
Professor Perry compared the number of medical school graduates with the current year population. I think a better comparison is the current year medical school graduates and the number of live births 26 years earlier.
The number of live births in the U.S. declined 24% from 1955 to 1975. If all else were equal, the number of medical school graduates should have declined 24% from 1981 to 2001. But the number of graduates actually increased by 3%.
larry-
the issue is not with the tort settlements so much as the 700bn-$1 trillion spend trying to avoid them.
http://www.washingtonpost.com/wp-dyn/content/article/2009/07/30/AR2009073002816.html
methinks: "If being a doctor is so rewarding, wouldn't you expect at least the same percentage of the population to opt for medical school?"
Not in the 1980s and 1990s. The demand for high quality financial MBAs and for computer scientists skyrocketed in those two decades. I believe the demand for highly trained engineers did as well. IMO, the path to high salaries in those fields was much easier than going through the 9 to 12 years of training required to become a medical doctor. It was simple competition for talent.
methinks: "Why would that be? IQ's are genetically determined . As a percentage of new births, they should have remained about the same."
I'm not sure that last sentence is true, either. Suppose that, in the 1970s and 1980s, women with high IQs had a lower fertility rate than women with lower IQs. Then the percentage of live births with genetically determined high IQs should decline. I do not have the data with me right this minute, but I've seen evidence that this was exactly the case not just in the U.S. but worldwide.
"I do not have the data with me right this minute, but I've seen evidence that this was exactly the case not just in the U.S. but worldwide."
Wow, the idiocracy is nigh.
No idea what you mean, Paul.
Consider reading How the World's IQ is in Decline
jet-
i would go even further and dispute that IQ's are genetically determined.
to be sure, there is a genetic component, but how you are raised, taught, encouraged to learn and think etc matters a great deal too.
calling it a pure genetic lottery is totally inaccurate.
nurture is a key issue as well, perhaps even a more important one as you look at overall achievement.
a change in child rearing patterns could yield far bigger effects than simple idiocracy style breeding quantity divergence.
jet-
have you seen the movie to which paul is referring (idiocracy)?
if not, you should. its central premise is precisely the trend toward breeding rate divergence to which you linked.
it's hilariously funny and darkly prophetic.
morganovich,
That's an extremely controversial topic, and has been all my life. Evidence exists to support both genetics and environment as determinants of IQ.
The link I just provided mentions both genotypic intelligence (inheritable) and phenotypic intelligence (environmental). It's a short piece - 640 words. Did you read it?
morganovich: "but how you are raised, taught, encouraged to learn and think etc matters a great deal too."
Based on evidence I've read, I do not believe those factors affect raw IQ. But many smart people have agreed with you.
I do believe that poor nutrition - especially early childhood nutrition - can inhibit development of intellect.
This comment has been removed by the author.
jet-
"I think a better comparison is the current year medical school graduates and the number of live births 26 years earlier. "
why is that a better comparison? it might tell us about % of people interested in medicine, but it does not tell us about the supply of doctors relative to the overall population and thus demand.
if demand were high (and the rewards system were not so badly distorted) you's expect salaries to rise and supply with it if demand were up from population dynamics.
it's the size of the over 65's that really drives demand for healthcare.
the size of the birth cohort that would be graduating now is less of a big deal.
we have more software engineers and fewer farmers than we use to in absolute and % terms. it's driven by demand, not the size of the birth group.
there is little reason to suspect that in a functioning market, %'s going into careers would stay constant. such shifts ought to offset population dynamics in high demand occupations. (unless, of course, you mess with the market dynamics to queer the incentives or act ologopolistically around supply etc)
i have no real idea on how much we can blame the AMA vs the fact that the market is a morass of insurance issues, bad incentives, federal and state interference, and liability and all of the above may well be true, but i doubt a small birth group in the 70's is having a major impact on doctor supply.
i suspect this is driven more by the fact that doctors earn less than they used to, work in less satisfying ways, and have to deal with an outlandish regulatory and accreditation thicket.
personally, i cannot see why anyone would chose it as a career for business reasons. the initial investment, opportunity cost, and ultimate payscale are really unattractive and made far worse after tax as getting your comp in salary gets you drilled come april.
i know a bunch of docs that have gotten out of practicing because they said they could not make a good living doing it.
i suspect that is the biggest driver.
morganovich: "nurture is a key issue as well, perhaps even a more important one as you look at overall achievement."
Achievement is certainly very different from IQ.
Are you asserting that the environmental factors you listed are more important than genetics in determining academic and economic achievement? If so I agree with you.
Are you arguing that the environmental factors you listed are more important than genetics in detemining IQ? If so, I definitely disagree with you.
morganovich: "the size of the birth cohort that would be graduating now is less of a big deal"
I completely disagree. Medical schools only accept applicants who have both very high intelligence and extremely high levels of academic achievement.
If you read my several comments carefully, you wold note that:
1. the supply of individuals with very high intelligence declined by at least 24% from the Baby Boom years to the Baby Bust years;
2. the competition for highly intelligent persons increased significantly at exactly the time when the Baby Bust generation reached college age.
All else equal, we should have expected a decline in medical school graduates from 1981 to 2001. But we actually saw a small increase.
morganovich: "if demand were high (and the rewards system were not so badly distorted) you's expect salaries to rise and supply with it if demand were up from population dynamics."
Supply of physisians could rise only if the demand for all other professions remained constant or if the potential supply of physicians increased dramatically But that's not at all what happened.
First, the supply of highly intelligent 20 to 30 year-old Americans declined in the 1990s - pure and simple - due to the baby bust of the 1970s.
The demand for young, highly intelligent Americans skyrocketed at the very same time - the demand for computer scientists, for financial experts, for PhD electrical engineers and scientists.
Those supply and demand factors were present not just in the U.S. but worldwide.
one example? How about the VA and DOD hospitals who can pull up virtually any serviceman's medical history if he is at their facility?
and how about the bulk prescription drugs that the VA can negotiate for also as a cost savings?
If you could go to ANY doc-in-box when you got sick and pay 1/2 or less what you'd pay to see a primary care and probably in 1/10 the wait time and that doc-in-the-box could see your medical history..
would that empower you to take advantage of a more open marketplace where you might even be able to shop around first before you selected?
Could you take care of your own routine health care needs by first seeing a doc-in-box before you went through the expense and trouble to wait to see a Primary Care?
electronic medical records would allow you to change docs easily whenever you wanted.
they very much would empower you to have more choice and more options.
Genetics is not the only determinant of IQ, but genetics play a large role.
I buy Jet Beagles argument that there there was reduction in children born to high-IQ mothers. But, I guess I was thrown off by Jet Beagle's assertion that it was the bust that caused a reduction of high IQ's. It would argue it was the birth control pill that allowed women with higher opportunity costs to avoid having children.
Something to consider is that while the number of immigrants (legal) grew at three times the rate of the overall annual population growth. I don't know what that does to for the pool of available doctors.
jet-
i helped a professor develop iq tests in college as a way to earn beer money.
we used to discuss the n vs n think all the time.
"raw iq" as you describe it is a pretty fraught concept. it's not really clear just what that is and studies to try and get at this come up with outlandishly different results.
take a look at the attribution levels on pgs 40 or so.
http://www.econ.nyu.edu/user/bisina/Chapter5_Sacerdote.pdf
the attribution %'s vary from .19 to .88 depending on the study. that's so wide as to amount to zero consensus.
brains have deep nerual plasticity. they develop in response to patterns and stimulus.
think of it like an fpga. you may be born with a ton of gates and a high bus speed, but how those gates get programmed winds up being critical to what you can do.
i think this "either or" debate about nature vs nurture has been foolish from the start. both are big factors. my suspicion is the folks trying to prove it is juts one or the other are just dogmatic zealots trying to claim that their specialty is the only one that matters.
"Supply of physisians could rise only if the demand for all other professions remained constant or if the potential supply of physicians increased dramatically But that's not at all what happened."
sure, which is why i made the point that a lot of that might eb a result of poor relative payscales, high relative initial investment and opportunity costs, and a perception that the field is in decline hamstrung by regulation and interference.
" so which is it?
Both. The two are not mutually exclusive.
M & M causes costs to rise as more and more people become part of the system. The demand for services rise, causing prices to rise. Since patients do not bare the full cost of these services, they have no issue requesting tests and the like that they may not need. Costs rise."
But if Medicare holds firm on what it will reimburse doesn't that also help keep down prices?
It must if some docs say they cannot make money on Medicare and MedicAid patients and if they dump those patients and raise prices on their o their other folks - with private insurance (who also control costs) - how does Medicare and MedicAid get the blame even when private insurers are in the game also?
" That's right, Larry. You are now face to face with the defining characteristic of government-run programs (not just THIS government's programs, mind): You pay more to get less.
Where there is competition and government and third party payers are NOT involved, you continue to get more for less."
and I've asked you out of over 200+ countries in the world is there not at least one example of what you are advocating?
name 3 countries that do what you advocate doing in this country.
surely there are 3 countries out of 200 that do more/better than govt-run countries....
"But if Medicare holds firm on what it will reimburse doesn't that also help keep down prices?"
no. it creates rationing which increase price in other ways (long waits, unavailable service, less supply, etc)
look at what caps on food prices did to food supply and availability in venezeula.
what will happen is that fewer and fewer docs will take M+M, especially new patients.
this will reduce the value of M+M insurance and cause those who have it to need to buy supplemental insurance or pay cash for what they need (or go without).
that does not sound like keeping prices low to me.
morganovich: "i think this "either or" debate about nature vs nurture has been foolish from the start. both are big factors. my suspicion is the folks trying to prove it is juts one or the other are just dogmatic zealots trying to claim that their specialty is the only one that matters."
Well, I definitely disagree with your characterization of those "folks" as "dogmatic zealots".
" that does not sound like keeping prices low to me."
in other countries that have Medicare for all - UHC - MRI's and other diagnostics and therapies are far, far cheaper.
Are there no countries in the world that do not have govt-controlled HC and instead a free-market type system?
200 countries.. maybe 50 have UHC, that leaves 150 countries that have some kind of a system other than govt healthcare , no?
morganovich: "i think this "either or" debate about nature vs nurture has been foolish from the start. both are big factors. my suspicion is the folks trying to prove it is just one or the other are just dogmatic zealots trying to claim that their specialty is the only one that matters."
+1
AKA, vested interests and ideologues are alive & well. It's not different this time.
morganovich: "which is why i made the point that a lot of that might eb a result of poor relative payscales, high relative initial investment and opportunity costs, and a perception that the field is in decline hamstrung by regulation and interference."
Those are all plausible explanations. But that doesn't mean at all that the decline in medical school graduates per 100,000 population cannot have a much simpler explanation: demographics.
Professor Perry argued:
the restriction on the supply of doctors relative to a growing population is one example of the "power of organized medicine".
He may be correct. But I have provided evidence that the power of women to reduce their fertility - the power of birth control after the mid-1960s - restricted the potential supply of doctors in the 1990s.
"in other countries that have Medicare for all - UHC - MRI's and other diagnostics and therapies are far, far cheaper."
and they have 9 month waits to get them.
cash cost is not the only price.
if price is too low, you get rationing and fail to generate supply.
the best price performance HC system in the world is singapore. their system is nearly all cash pay with insurance only for real disasters and that applies only after you have spent what is essentially your HSA.
granted, they require you to put money into the hsa's, but that feature is not what drives price/peformance. what makes it work well is that you pay for only what you really feel you need (user pays) and have incentive to shop around for the price/quality level that looks best to you.
" if price is too low, you get rationing and fail to generate supply"
we have rationing already in this country from private providers who will not approve an MRI at all unless they think it is appropriate.
Not sure how hospitals make that call for charity cases..perhaps every MRI they sell to a charity case is money in the pocket on cost-shifting?
re: Singapore
Would you support that in this country?
I would.
I "get" what you are after.
I even AGREE believe it or not.
I just think what we have now is not sustainable and there is nothing else on the table as a competitive alternative.
I've asked before.
what is the rationale for the IRS to disallow health care costs up to 7.5% of your AGI?
what's the rationale?
jet-
"
He may be correct. But I have provided evidence that the power of women to reduce their fertility - the power of birth control after the mid-1960s - restricted the potential supply of doctors in the 1990s."
but lots of lucrative careers have seen increases, not decreases. we get more lawyers, more biz school grads, etc.
this seems to make the demographics argument look questionable.
why would it affect doctors but not lawyers and biz school grads?
the same demographics apply to all.
something about doctors is causing them to behave differently than other grad school driven careers.
this is why i find the "incentives" argument more persuasive. this does not prove mark's thesis about this being the work of the AMA and i'm not really sure how to separate that out, but we can get a sense on the demographic argument by looking at other career choices that require grad school, and those seem to be running contrary to what your demographic thesis would indicate.
larry-
"we have rationing already in this country from private providers who will not approve an MRI at all unless they think it is appropriate."
that's a wild straw man. virtually all plans will approve an mri in most cases. i have had several. however, your argument favors letting users decide what is appropriate and pay for it themsleves taking the insurer out.
what i support is for all americans to be allowed (but not required) to put cash tax free into HSA's and use it as they see fit.
i support the complete abolition of medicare and medicaid as they exist and moving them to block grants of cash.
i favor complete deregulation of health insurance to allow companies to compete across state lines and to offer whatever plans at whatever price they and their customers agree upon and a move toward making health insurance like other forms of insurance: rarely used. and for exceptional circumstances.
most us healthcare should be cash pay.
"we have rationing already in this country from private providers who will not approve an MRI at all unless they think it is appropriate."
that's a wild straw man. virtually all plans will approve an mri in most cases. i have had several. however, your argument favors letting users decide what is appropriate and pay for it themsleves taking the insurer out.
well no. I'm only pointing out that the insurer - whether govt or non-govt denies treatment - i.e. rations.
what i support is for all americans to be allowed (but not required) to put cash tax free into HSA's and use it as they see fit.
is this not already the case?
i support the complete abolition of medicare and medicaid as they exist and moving them to block grants of cash.
Part A is mandatory, funded from payroll taxes. Part B is totally voluntary but heavily subsidized.
What Part B offers that is most important is guaranteed access and the same premiums for everyone.
Why no remove the subsidy and sell it for what it costs to provide the program but maintain guaranteed access and community premiums?
i favor complete deregulation of health insurance to allow companies to compete across state lines and to offer whatever plans at whatever price they and their customers agree upon and a move toward making health insurance like other forms of insurance: rarely used. and for exceptional circumstances.
is making it available across state lines a violation of states rights and the imposing of a Federal government dictate that rolls over states rights?
most us healthcare should be cash pay.
you are opposed to insurance ?
morganovich: "why would it affect doctors but not lawyers and biz school grads?"
In the first place, the quality standards are nowhere near as high. The AMA does control those standards for physicians, so Dr Perry is correct that AMA did control the supply of physicians by not reducing its standards.
Law school takes about 33 months. An MBA can be obtained parttime or in 18 to 20 months fulltime. It takes 5 to 6 years beyond undergraduate school to become an independent physician.
Highly intelligent persons realized they could achieve high incomes from less demanding careers. Why defer gratification for an additional 3 to 4 years? Why work 80 hours a week as many interns are required to do?
"
well no. I'm only pointing out that the insurer - whether govt or non-govt denies treatment - i.e. rations."
and i am pointing out that that is not true. those with a need get service rapidly. it is not "rationing" to set out in a contract what is and is not covered.
"
is this not already the case?"
not, it's not. many state put dramatic limits on this and it's only legal if you subscribe to certain plans and pay for the privilege.
"Part A is mandatory, funded from payroll taxes. Part B is totally voluntary but heavily subsidized.
What Part B offers that is most important is guaranteed access and the same premiums for everyone."
what part b offers is the preposterously ruinous sale of dollars for about 13c. of course it's attractive to seniors. who doesn't like buying things for 87% less than they cost?
but that's precisely why it is not a viable system.
"
you are opposed to insurance ?"
in its current form, yes.
http://youtu.be/I7pqRjHQ9BU
watch the video.
health "insurance" is not insurance at all. it's a buffet. it is the cause of most of the problems.
"
In the first place, the quality standards are nowhere near as high. The AMA does control those standards for physicians, so Dr Perry is correct that AMA did control the supply of physicians by not reducing its standards."
so do state bad associations.
if this issue is just about demographics, you'd see it in lawyers too. but you do not.
"It takes 5 to 6 years beyond undergraduate school to become an independent physician.
Highly intelligent persons realized they could achieve high incomes from less demanding careers. Why defer gratification for an additional 3 to 4 years? Why work 80 hours a week as many interns are required to do?"
this is precisely the argument i made above: that it is cost/benefit and incentive based.
it sounds like you are agreeing with me and moving away from the demographic explanation.
is that the case, or am i misunderstanding you?
"is making it available across state lines a violation of states rights and the imposing of a Federal government dictate that rolls over states rights?"
no. that's actually precisely what the commerce clause is for: to prevent states from erecting tariffs and NTB's against each other.
sorry, bar associations, not bad.
freudian slip there.
Larry G: "is making it available across state lines a violation of states rights and the imposing of a Federal government dictate that rolls over states rights?"
The U.S. Constitution gave Congress the responsibility to prevent restriction of interstate commerce. It is exactly the restriction on interstate trade of goods and services which our nation's founders sought to prevent. As a result of their foresight, you are able to buy goods (and services) from another state and have them shipped to (or applied in) your home state.
Unfortunately, the U.S. Congress enacted an exception for health insurance: the 1945 McCarron-Ferguson Act.
"
well no. I'm only pointing out that the insurer - whether govt or non-govt denies treatment - i.e. rations."
and i am pointing out that that is not true. those with a need get service rapidly. it is not "rationing" to set out in a contract what is and is not covered. "
come on Morg have you not seen news reports or seen personally situations where a private provider DENIED coverage?
"is this not already the case?"
not, it's not. many state put dramatic limits on this and it's only legal if you subscribe to certain plans and pay for the privilege.
HSAs at the Federal Level?
what part b offers is the preposterously ruinous sale of dollars for about 13c. of course it's attractive to seniors. who doesn't like buying things for 87% less than they cost?
it's grotesquely under-priced I totally agree.
People with 3 houses and 5 cars pay 100 a month for health care.
but that's precisely why it is not a viable system.
why not price it for what it costs but insure that everyone can buy it?
"you are opposed to insurance ?"
in its current form, yes.
http://youtu.be/I7pqRjHQ9BU
watch the video.
cute video... and on target but isn't this a private sector problem also?
would you have govt "fix" this rather than the marketplace?
health "insurance" is not insurance at all. it's a buffet. it is the cause of most of the problems."
we actually agree more than we disagree.
but you are talking about private sector insurance here also, right?
would you take away the employer-provided health care and let everyone seek insurance on their own?
What "constitution"?
That and an ability to parse words and torture logic should get me appointed to a lifetime of deciding that congress can do whatever it wants to the serfs it owns.
Oh Jesus H. Keerist
don't you mean ALL governments and not just the US?
are you not opposed to all types of government in reality?
larry--
"
come on Morg have you not seen news reports or seen personally situations where a private provider DENIED coverage?"
that is a nonsense argument.
you sign a contract that lays out your coverage. what it says is what you get. calling that "denying" coverage is like claiming your car insurance company should pay for your crash into a tree even though you on;y bought liability coverage.
you are trying to call contracts rationing. it's just not so.
"
why not price it for what it costs but insure that everyone can buy it?"
because that leave all the problems of cost spirals, users not facing their own costs etc.
"
cute video... and on target but isn't this a private sector problem also?
would you have govt "fix" this rather than the marketplace?"
no. you get the government out of the system. period. this is not a private sector problem. it's a problem driven by requirements and bad tax policy.
there is no "private sector insurance" in the way that you mean. it's provided by private companies, but subject to so much federal and state regulation that it is not a real market.
"What "constitution"?
That and an ability to parse words and torture logic should get me appointed to a lifetime of deciding that congress can do whatever it wants to the serfs it owns."
yup.
constitutions only work if you follow them.
you sign a contract that lays out your coverage. what it says is what you get. calling that "denying" coverage is like claiming your car insurance company should pay for your crash into a tree even though you on;y bought liability coverage.
you are trying to call contracts rationing. it's just not so.
we're talking about the small print that changes often, right?
govt has the same thing.
both pvt and govt deny coverage.
are you saying that if they tell you up front, it's not rationing?
"
why not price it for what it costs but insure that everyone can buy it?"
because that leave all the problems of cost spirals, users not facing their own costs etc.
isn't that how all insurance works essentially?
"
cute video... and on target but isn't this a private sector problem also?
would you have govt "fix" this rather than the marketplace?"
no. you get the government out of the system. period. this is not a private sector problem. it's a problem driven by requirements and bad tax policy.
so everyone should be able to exclude from taxation any/all health care expenditures?
there is no "private sector insurance" in the way that you mean. it's provided by private companies, but subject to so much federal and state regulation that it is not a real market.
are there any countries where that is not true?
not a loaded question - an honest one.
are there any truly "real" health insurance "markets"?
I'm sure you are aware that Medicare does not cover people who go abroad, right?
Is there insurance - in the world - that is not restrained by the govt where you live?
Which is to say they don't work, Morganovich.
The people whom it restrains are the same ones who get to decide. The only thing that works is competition.
Most small countries try to compete for productive people by reducing the burdens on them. They have no choice, they don't have a Department of Involuntary Servitude (IRS) to hunt down their citizens to the end of the earth. They don't try to ban ex-pats for leaving because they didn't want to be robbed by them. Campione has not taxes. Swiss Cantones compete for business internally and from abroad etc., etc.
There are significant downsides to being a citizen of a superpower once the government grows this large and intrusive.
BTW, did you buy in Nevis or are you planning to reside on St. Barth's?
larry-
"are you saying that if they tell you up front, it's not rationing?"
yes. it's called a contract. you decide what you want to buy, pay for it, and get it. that's the way any market works. you act like the insurers get to decide after the fact. they do not.
you could try the tortured logic of calling anyhting with a price "rationed", but that's just a semantic game. hammers are then "rationed" too as are babysitters etc.
"
isn't that how all insurance works essentially?"
no. insurance covers extreme events. your car insurance does not cover oil changes, gasoline, and getting the car waxed. your homeowners insurance does not cover your dishwasher breaking.
"so everyone should be able to exclude from taxation any/all health care expenditures?"
do you even read what others write before you ask stuff like this? are you seeking to be deliberately difficult or are you really just not grasping this?
"
are there any countries where that is not true?
not a loaded question - an honest one.
are there any truly "real" health insurance "markets"?"
who cares? why is this a relevant criteria for anything? there sure used to be.
but, like education, healthcare has become s complete mess because it has been so interfered with.
markets work. why is healthcare some special case?
"There are significant downsides to being a citizen of a superpower once the government grows this large and intrusive."
a government powerful enough to give you everything you want is powerful enough to take everyhting you have.
our constitution did work for a while (and is still better than most). the civil war did a great deal of harm, and FDR really did the rest. you need to guard them vigorously from such outrages. our failures then led to the mess we have now.
"BTW, did you buy in Nevis or are you planning to reside on St. Barth's?"
my 2nd passport is from st kitts, not nevis, though they are confederated.
i own no property there.
a kittician passport lets you live and work visa free anywhere in the former british commonwealth and the whole carribean community.
this includes canada, england, ireland, austrailia, etc.
that's part of what makes it so potentially attractive. you do not need to live on a little rum soaked island. so long as i left my business offshore, i could, for example, move to vancouver and pay no income tax.
"are you saying that if they tell you up front, it's not rationing?"
yes. it's called a contract. you decide what you want to buy, pay for it, and get it. that's the way any market works. you act like the insurers get to decide after the fact. they do not.
but govt insurance tells you also what is not covered. Medicare tells you up front that there is a 20% deductible and they won't cover dentists and optometrists.
"you could try the tortured logic of calling anyhting with a price "rationed", but that's just a semantic game. hammers are then "rationed" too as are babysitters etc."
well no... I'm just saying that both private and public insurance have lists of things they won't cover and criteria for what they will cover ...
"
isn't that how all insurance works essentially?"
no. insurance covers extreme events. your car insurance does not cover oil changes, gasoline, and getting the car waxed. your homeowners insurance does not cover your dishwasher breaking."
true.
"so everyone should be able to exclude from taxation any/all health care expenditures?"
do you even read what others write before you ask stuff like this? are you seeking to be deliberately difficult or are you really just not grasping this?
no, I read guy. I'm asking your view. Are you in lockstep with others on these things? I hope not.
"
are there any countries where that is not true?
not a loaded question - an honest one.
are there any truly "real" health insurance "markets"?"
who cares? why is this a relevant criteria for anything? there sure used to be.
well because if there are existing markets in the world, if nothing else it shows that it can be done and is being done right now.
"but, like education, healthcare has become s complete mess because it has been so interfered with."
in the industrialized countries for sure.
there are over 150 other countries that do not have near as much govt influence.
Not all of those countries are "poor" and primitive. some actually attract expats.
markets work. why is healthcare some special case?
because people with health care needs are sometimes like people who have had multiple accidents and cannot get auto insurance.
what do you do with people the private sector will not insure?
i could, for example, move to vancouver and pay no income tax.
and then come to the nasty govt controlled US for healthcare?
:-)
Does St. Kitts have UHC or is it market ?
Roosevelt and then Obama finished it off. but, yes, Roosevelt. I don't think it's pretty good anymore.
You can do it without buying property. I just wondered if you took that route.
As a former citizen, you do have to pay taxes on any income earned in the U.S. I don't know if this means income earned trading securities on U.S. exchanges.
How bad will it have to get for you to pull the trigger?
morganovich: "it sounds like you are agreeing with me and moving away from the demographic explanation.
is that the case, or am i misunderstanding you?"
You misunderstand me. I'm defintely not moving away from the demographic argument.
The absolute number of potential new physicians in any year is limited by the combination of:
1. the number of live births (and the percent of those which are highly intelligent) 26 years earlier;
2. the decision by AMA to not reduce the quality of medical school students.
The first part is the demographic argument I made earlier. I never argued it was the only factor (though I think it is the most important one).
The demand for those persons who can be physicians - the highly intelligent persons - is not just the demand for physicians. It is also the demand for PhD scientists, financial wizards, highly intelligent lawyers (subset of all lawyers) and other professions which have increased faster than the population has grown.
Demographics alone suggest that the U.S. should have had fewer medical students in the 1990s than in the early 1980s. The population of highy intelligent persons in their 20s declined. But the number of medical students actually increased slightly - despite the demographics, despite the competing demands for highly intelligent persons, despite the disincentives for entering the medical field which you described.
The AMA may well be the strongest trade union in the U.S. But there are several other explanations - including and especially demographics - for why the number of medical students did not keep up with the population growth.
and then come to the nasty govt controlled US for healthcare?
Unlikely. Canadians come here for health care because it's so much better and more available (which should be a clue to you, but somehow isn't) U.S. healthcare will deteriorate, so Morganovich will likely seek a private option abroad. Moreover, it's likely that an a rich ex-citizen will get on the black list that prevents the issue of a visitor's visa. He is unlikely to be able to get back into the country. If you have so much as two dimes to rub together, the USA retaliates against you for leaving.
jet-
if demographics are the key issue as opposed to cost/benefit and competing opportunities, then why did this trend not show up with lawyers?
i am not making an ama argument, i'm making the argument that there were just better cost/benefit opportunities.
if lawyers can overcome the demographic issue and doctors cannot, this would seem to argue that the key factor is attractiveness of the profession, not demographics.
larry
"
and then come to the nasty govt controlled US for healthcare?"
are you seeking to be odious and obtuse or do you really not get this?
One thing not touched on in this discussion is whether the supply of physicians needed to increase as the population increased.
Despite the enormous growth of the manufacturing output in the U.S., the number of factory workers has declined significantly. That's because the productivity of factory workers has soared as tasks were automated. Productivity of agriculture workers has likewise soared.
Has the productivity of physisicians also increased since the 1970s? I think it has.
I know that surgeons have become more productive. My wife, an OR nurse, has explained over the years how complicated surgeries requiring long recovery times have been simplified. She has shown me equipment which sharply reduced the delays which the OR used to face waiting for lab results on tissue samples. My wife has explained how innovations in OR equipment setup have reduced surgeon idle time between cases.
Dr Perry's graph actually indicates an increase in productivity by America's physicians. Are we sure that's a bad thing?
"
but govt insurance tells you also what is not covered. Medicare tells you up front that there is a 20% deductible and they won't cover dentists and optometrists."
and this has what to do with anyhting? there is no logic behind your thoughts here.
federal health programs are not contracts in any true sense as the one paying the costs is not the one getting the goods and such payment is not voluntary.
"
no, I read guy. I'm asking your view. Are you in lockstep with others on these things? I hope not."
no, you are asking the same questions over and over and seem unable to understand the answers.
"
because people with health care needs are sometimes like people who have had multiple accidents and cannot get auto insurance"
this is easily solvable by having health insurance act like real insurance and most day to day health issues being cash pay, just like your car.
there even already exists setf of "condition change" insurance where you pay a small about to have higher premiums for your actual insurance covered if your health deteriorates later.
your argument is not a reason and it's nothing like an argument for insurance over cash grants if you wish to help those in need.
what do we do with people who cannot afford food larry?
do we give them some cash and let them shop or do we give them an amex black card and turn them loose at whole foods and nobu?
if we did the latter, do you think food stamps might rise in price?
you seem to feel healthcare is some sort of right.
it's not. it cannot be.
you cannot have a right that forces others to give you things.
morganovich: "why did this trend not show up with lawyers?"
Oh, come on. I already explained this. Law schools in general do not have nearly as high standards as do medical schools (though a small few do). A very high IQ is not a prerequisite for law school. The potential supply of lawyers is much, much greater than the potential supply of physicians.
"Dr Perry's graph actually indicates an increase in productivity by America's physicians. Are we sure that's a bad thing?"
that's actually a really interesting point.
with better tools, procedures etc and a big move toward outpatient surgery etc and home monitoring of conditions there is no reason to suppose that doctors have not become more productive.
this does make the doctor to population ratio look like a questionable indicator to determine the availability of healthcare.
apply this logic to farmers, and one would think we'd be starving by now.
Jet,
Innovations in medicine have certainly made doctors more productive. But, there are still shortages of certain types of doctors. So, maybe we don't need as many, but it seems we need more than we have.
" Unlikely. Canadians come here for health care because it's so much better and more available (which should be a clue to you,"
not that many Canadians. Most Canadians are just fine with having healthcare; they'd have none if they lived in the US.
"but somehow isn't) U.S. healthcare will deteriorate, so Morganovich will likely seek a private option abroad. Moreover, it's likely that an a rich ex-citizen will get on the black list that prevents the issue of a visitor's visa. He is unlikely to be able to get back into the country. If you have so much as two dimes to rub together, the USA retaliates against you for leaving"
so Morg will seek true free market healthcare? So it really does exist?
"
Oh, come on. I already explained this. Law schools in general do not have nearly as high standards as do medical schools (though a small few do). A very high IQ is not a prerequisite for law school. The potential supply of lawyers is much, much greater than the potential supply of physicians."
i disagree.
what evidence do you have that doctors are smarter than lawyers? most of med school is rote memorization. my friends who do medical research refer to doctors as "plumbers" and mock them for being too dumb to do or even understand research. (of course, there is likely some bias there)
i have not found doctors, especially GP's to be particularly bright in comparison to many other professions. to be sure, some are, but many are not.
you seem to be making a very large assumption there.
i have no idea what level of credibility to place on a study like this: (likely not much)
http://pieceofmind.wordpress.com/2008/11/25/but-where-do-bloggers-fit/
but to look at it, legal occupations look a great deal like md equivalents. the bar extends a bit further left, but it includes folks like paralegals. this is not just those admitted to the bar whereas the one for doctors is MD+.
i have real doubts that the talent pool is all that different, though if you have some data there, please share it.
"not that many Canadians. Most Canadians are just fine with having healthcare; they'd have none if they lived in the US."
every part of this is wrong.
they are not fine. the waits are horrendous and you come to the us the minute you get anyhting complicated.
they can (and do) buy insurance here. they can pay cash. you make this strangle leap from "no universal coverage" to "no healthcare".
you do not have toothbrush insurance. is that stopping you from getting one?
"so Morg will seek true free market healthcare? So it really does exist?"
seriously, what is the point of a question like this?
healthcare would be better if it were free market. you keep your pay and spend it as you like on procedures that would be better and cheaper than they are today.
we could get far more care for the same money, or the same care for less money.
either way is a win.
seriously, what is the point of a question like this?
pretending at intellect.
Well I was in Canada recently and the folks I talked to totally disavow this.
They LIKE their healthcare and they LIKE the fact that they can move from job to job without having to worry about healthcare.. it stays the same.
" they can (and do) buy insurance here. they can pay cash. you make this strangle leap from "no universal coverage" to "no healthcare"."
children who come down with serious condition are not toothbrushes.
they can be denied coverage or denied insurance in the US. That never happens in Canada.
Universal Coverage means you and your family are never denied coverage and you never have to go the ER to get care because you cannot afford a doctor.
There are pluses and minuses no doubt but the vast majority of people who live in countries with UHC PREFER it to the US system where the "wait times" for those who can't get insurance is infinite.
In Canada you don't see gallon jars in the 7-11s begging for help for a child's operation.
If you gave the choice of UHC to Americans - half or more would take it.
If you advocating repealing EMTALA - would you ever get elected?
As far as I know there is not a single politician who openly advocates EMTALA which is for all practical purposes really expensive universal coverage and long "wait" times but available to everyone.
What we both agree on is that our current system SUCKS - so that's a start eh?
"children who come down with serious condition are not toothbrushes."
but goods and services are goods and services. they all obey the same rules. insurance raises prices and creates moral hazard around payment.
re canada:
http://www.globalnews.ca/canadian+health+care+system+fails+vulnerable+report/6442461539/story.html
the system totally fails you if anyhting complex happens.
it's also nearing BK.
http://nostrums.blogspot.com/2010/06/canadas-bankrupt-health-care-forced.html
i do not agree that our current system sucks. the us has great healthcare, far better than canada's.
it could be a lot better, but if you get cancer, you want to be here, not canada or the eu.
where we differ is that you seem to think if we only emulated the failing system to the north, it would work.
just like with education, our problem is not our helthcare system, it is government interference in that system.
remove that, and the system will improve itself dramatically in short order.
morganovich: "the bar extends a bit further left, but it includes folks like paralegals. this is not just those admitted to the bar whereas the one for doctors is MD+."
Well, you may be correct. The chart contained in your link is the same one I've looked at. I didn't realize the "Legal Occ" group might contain paralegals. Or that the "Medical Occ" did not contain Registered Nurses, Nurse Practitioners,Physician Assistants, or other highly trained medical occupations. Actualy, I'm not sure either of us can know for certain what is represented by that chart.
If I find other data, I'll let you know. I've read before that MD's had the highest IQs, but it's possible that information was based on the same study.
methinks: " there are still shortages of certain types of doctors."
If you are referring to General Practitioners, I think that's a problem where the AMA does exert its muscle. I've read many times that Nurse Practitioners could perform many if not most of the tasks retricted to General Practitioner MDs.
Of course, part of the problem with a GP shortage in rural areas is likely due to Medicare reimbursements. A free market would ensure that MDs in rural areas receive enuogh compensation to make the work attractive.
"children who come down with serious condition are not toothbrushes."
but goods and services are goods and services. they all obey the same rules. insurance raises prices and creates moral hazard around payment.
any/all insurance no matter what? Is that an argument against any/all insurance?
re canada:
http://www.globalnews.ca/canadian+health+care+system+fails+vulnerable+report/6442461539/story.html
the system totally fails you if anyhting complex happens.
dueling articles:
Poll: Canadians like their health care despite grumbles
http://www.mcclatchydc.com/2009/07/21/72229/poll-canadians-like-their-health.html
it's also nearing BK.
http://nostrums.blogspot.com/2010/06/canadas-bankrupt-health-care-forced.html
i do not agree that our current system sucks. the us has great healthcare, far better than canada's.
it could be a lot better, but if you get cancer, you want to be here, not canada or the eu.
even if you do't have insurance?
where we differ is that you seem to think if we only emulated the failing system to the north, it would work.
nope.
I'm just skeptical that your "free market" model "works" for health care and that UHC is better for people even in flawed implementations compared to a system where people have no insurance at all.
Even auto insurance would dump high risk if the govt did not require otherwise.
If we had true free-market auto insurance, we'd have tons of people driving around without insurance...
when you have a system where the folks who don't have insurance still have their costs paid for by others - it's not really a free market system - but that describes every industrialized country on earth - right?
We have a system where people who do not have insurance are paid for by others - right?
we have a law - EMTALA that requires hospitals to treat anyone no matter if they have insurance or not and the hospitals then bill you for that care.
and you say we have a good system?
but you don't really because you want to change it and make it even less available to those who cannot afford insurance.
Would you support the repeal of EMTALA?
"But if Medicare holds firm on what it will reimburse doesn't that also help keep down prices?"
No, it helps keep down the number of doctors who will accept M&M patients.
If everyone "holds firm" on what they are willing to pay for watermelons, what do you suppose will happen?
"Holding firm" indicates lower demand. What happens to supply?
Supply and demand, Larry, immutable law.
"Holding firm" indicates lower demand. What happens to supply?
Supply and demand, Larry, immutable law.
friendly amendment - immutable theory not often found in a pure form in the wild.
What you are arguing is for health care costs to go up in order to assure supply.
this is in a country where we pay twice as much for health care already - is 16% of our economy and project to go to 30% if we do not reduce costs.
I do not see how you fix this by increasing costs....
the real immutable law here is that if we don't do something about health care costs - it will destroy our economy and that's not my opinion, it's the judgement of quite a few folks.
health care cost in other countries has essentially flat-lined and yes.. it's accomplished by "rationing".
we ration also - but pretend we do not.
when an insurance company chances the terms of your policy and reduces what they pay for and increases co-pays - that's essentially rationing.
Jet,
Yes, I was thinking mostly of GPs. There are some specialties experiencing shortages as well, but the shortage of GPs is the most pressing problem because of how Obamacare works.
"we have rationing already in this country from private providers who will not approve an MRI at all unless they think it is appropriate."
Unless you think people should determine for themselves when an MRI is called for, your comment makes no sense - as usual.
" Unless you think people should determine for themselves when an MRI is called for, your comment makes no sense - as usual. "
Nope.
I'm pointing out that others decide and they use criteria that some may interpret as "rationing".
Anytime a 3rd party decides you do not need an MRI, CT, etc is it considered "rationing"?
Say you got an MRI but you want another. If the insurance company turns you down (just like Medicare will also do) - is that "rationing"?
If ObamaCare turns down a request for an MRI is that "rationing"?
If Canada turns down an MRI is that rationing?
If Canada says you can have an MRI but must wait a month, is that rationing?
a week? two days?
" but the shortage of GPs is the most pressing problem because of how Obamacare works."
My current GP when I call gives me two appointment options.
One is for the Physician Assistant and the other to see her directly.
I still get to see her if the PA wants her to take a look.
I think it makes perfect sense.
Here's a question.
If more people are "covered" under ObamaCare will we still need all the ER staffing currently in place?
Where will the excess ER staff go ?
is the premise of ObamaCare that we'll need less ER folks and more GPs?
"well no. I'm only pointing out that the insurer - whether govt or non-govt denies treatment - i.e. rations."
Insurers deny reimbursment, not treatment. There's a difference. I doubt there's a limit to the number of MRIs you can get, unless there's a health risk, if you are willing to pay for them yourself.
" Insurers deny reimbursment, not treatment. There's a difference. I doubt there's a limit to the number of MRIs you can get, unless there's a health risk, if you are willing to pay for them yourself. "
this is a point I agree with in general but a "covered" treatment or diagnostic in much of the UHC world is what they will do or not do in rendering health care.
And if they deny it, it is said to be "rationing".
If Medicare denies a second MRI - and they will or MedicAid denies the first MRI (and they do), - some characterize this as "rationing".
but in the end - isn't it not that different from an insurance company that "covers MRIs" but denies a 2nd one?
the fine print says "if in our opinion the scan is "appropriate".
you are not guaranteed as many MRIs as you want - they essentially "ration" how many are provided for your paid coverage.
Methinks
"He is unlikely to be able to get back into the country"
Anymore, one can be pretty much anywhere they want to be electronically, so physical location seems less and less important.
Right now, it seems that morganovich travels the world while his body remains on life support in Utah. :)
And if they deny it, it is said to be "rationing".
That's right and for two reasons. That's not the promise of government healthcare and because for a long time (and in places like Canada to this day) a private market is illegal. So, if you are denied access to the government facilities, you cannot seek a private facility instead. This leaves people overpaying for substandard care or or no care at all (if you have to wait a year to get chemo, it's as good as getting no treatment and if you're turned down for dialysis, that's it.).
European countries have all had to reform their socialized medicine so that people have a free market option where they can get off wait lists by paying out of pocket.
Also, a necessary cost saving feature of universal care is that expensive but effective drugs were unavailable. Patients just didn't have access to them because the central planners decided they wouldn't be distributed in the system.
Socialized medicine makes decisions for you and you often don't have the choice to pay out of pocket. The reform that was necessary was to still make people pay for overly expensive, underperforming socialized medicine but give people a free market option where they can pay for the care they need out of pocket. There's also now private insurance and most countries leave that market pretty much unregulated.
There are at least two interesting facts to consider:
1.) Socialized medicine experiments have thus far been on small countries with small and relatively homogeneous populations. We are a 315 million person exceptionally homogeneous population. That matters both in terms of the exponentially large management issues, the difficulty of creating standardized rules governing care, and the cost of having to cater to such a large and diverse population. The closest example we have of a giant country administering to a large population is the Soviet Union.
2.) Even countries with tiny homogenous populations that are more like clubs than countries (Sweden, for instance), socialized care created wait lists and a lot of dissatisfaction. As Europeans are shifting away from dependence on failed socialized medicine to more privatized health care, our political overlords inflict it on us.
Anymore, one can be pretty much anywhere they want to be electronically, so physical location seems less and less important.
You're correct, Ron H. But, if you've lived in America for a long time you likely have dear friends you have to mentally prepare not to see until they visit you. Perhaps never again. If you're born in America to American parents, you probably have a lot of family here and that's a more difficult thing. Banishment is a tactic straight out of the Soviet playbook. I went through that kind of separation when we left the USSR and I can tell you that it's heart wrenching. It was an enormous loss. The 1996 Reed Amendment imposes this punishment on anyone who has had the temerity to achieve even a little success in the United States.
but in the end - isn't it not that different from an insurance company that "covers MRIs" but denies a 2nd one?
You are not denied a second MRI. You can pay for as many MRI's as you want.
Except maybe with medicaid. Medicaid has some very Draconian rules. If you don't accept the treatment medicaid is willing to pay for, you cannot pay the same doctor out of pocket. You have to start all over again with a new doctor and pay for it out of pocket. Nice way to treat the poor.
you are not guaranteed as many MRIs as you want - they essentially "ration" how many are provided for your paid coverage.
That's right. When you go to a restaurant and pay for a single entree you are not entitled to eat as many entrees as you want.
When you're talking about medicaid and medicare, you're not paying for any coverage. Someone else is paying for you and their willingness to provide you all you can eat medical care is zero.
Jet
"I've read before that MD's had the highest IQs, but it's possible that information was based on the same study."
You can bet it was written by an MD. :)
"they can be denied coverage or denied insurance in the US. That never happens in Canada."
But they are never denied timely treatment. That DOES happen in Canada
"friendly amendment - immutable theory not often found in a pure form in the wild."
Total nonsense.
"What you are arguing is for health care costs to go up in order to assure supply."
Again you demonstrate that you have no understanding of supply and demand.
Healthcare costs are what they are. You don't make them lower by not paying the full cost. Price controls don't work, Larry, You will get shortages, rationing, and poor service. There is no way around it. It's an immutable law.
"And if they deny it, it is said to be "rationing"."
Yet another concept Larry doesn't understand?
"What you are arguing is for health care costs to go up in order to assure supply."
No, you dim bulb. I'm pointing out that price controls don't work. You can't lower prices by refusing to pay the full cost. "Holding the line" on Medicare payments won't lower the cost of doctor visits.
Still intrigued by the question: "How many physicians should the U.S. have?"
Physicians per 10,000 population
Source: WHO, based on 2005-2010 data
Greece__________62
Russia___________43
Norway_________42
Switzerland______41
Spain___________40
Sweden_________38
Germany________36
Italy____________35
France__________34
Denmark________34
Ireland__________32
Australia________30
Belgium_________30
Netherlands_____29
Finland_________29
UK_____________27
United States____24
Poland_________22
Japan__________21
Mexico_________20
Canada_________20
Brazil__________18
Singapore_______18
China__________14
India____________6
That's right and for two reasons. That's not the promise of government healthcare and because for a long time (and in places like Canada to this day) a private market is illegal. So, if you are denied access to the government facilities, you cannot seek a private facility instead. This leaves people overpaying for substandard care or or no care at all (if you have to wait a year to get chemo, it's as good as getting no treatment and if you're turned down for dialysis, that's it.).
I'm not sure what "promise" you are talking about here. The basic promise if Universal Access. No one was ever promised unlimited health care no matter what.
"European countries have all had to reform their socialized medicine so that people have a free market option where they can get off wait lists by paying out of pocket."
and that's good. The purpose of UHC is not to provide any/all HC to any/all people. It's to establish a base level of care for all - and then if you want more and can afford more, then fine.
"Also, a necessary cost saving feature of universal care is that expensive but effective drugs were unavailable. Patients just didn't have access to them because the central planners decided they wouldn't be distributed in the system. "
huh? Don't the Europeans negotiate with the drug companies and we do not?
"Socialized medicine makes decisions for you and you often don't have the choice to pay out of pocket."
really? is this why Canadians pay extra for American care?
"The reform that was necessary was to still make people pay for overly expensive, underperforming socialized medicine but give people a free market option where they can pay for the care they need out of pocket. There's also now private insurance and most countries leave that market pretty much unregulated."
are you complaining here or what? If your complaint is that countries with UHC should allow people to buy "up" , I totally agree. I'd ask which countries forbid their people from buying "up"?
There are at least two interesting facts to consider:
1.) Socialized medicine experiments have thus far been on small countries with small and relatively homogeneous populations. We are a 315 million person exceptionally homogeneous population. That matters both in terms of the exponentially large management issues, the difficulty of creating standardized rules governing care, and the cost of having to cater to such a large and diverse population. The closest example we have of a giant country administering to a large population is the Soviet Union.
Jesus Keeerist - have you seriously looked at the list of countries with UHC and totaled up their populations? Most of the industrialized world has UHC. Your "small" claim is totally bogus.
"2.) Even countries with tiny homogenous populations that are more like clubs than countries (Sweden, for instance), socialized care created wait lists and a lot of dissatisfaction. As Europeans are shifting away from dependence on failed socialized medicine to more privatized health care, our political overlords inflict it on us."
I see no "shift". wishful thinking is more like it.
but in the end - isn't it not that different from an insurance company that "covers MRIs" but denies a 2nd one?
You are not denied a second MRI. You can pay for as many MRI's as you want.
I agree. But when Medicare tells you that - we say it is "rationing" and when your insurance company does it's not.
With Medicare some bean-counter is said to get between you and your Doc but private insurance does not have such bean-counters right? SIC!
"Except maybe with medicaid. Medicaid has some very Draconian rules. If you don't accept the treatment medicaid is willing to pay for, you cannot pay the same doctor out of pocket. You have to start all over again with a new doctor and pay for it out of pocket. Nice way to treat the poor."
MedicAid is our "Universal Health Care", right?
you are not guaranteed as many MRIs as you want - they essentially "ration" how many are provided for your paid coverage.
That's right. When you go to a restaurant and pay for a single entree you are not entitled to eat as many entrees as you want.
you can at an "all you can eat" place.
again - when Govt imposes that restriction - it's said to be "rationing" but when private insurance does, it's said to be "in the contract".
Govt healthcare also has a "contract".
In both cases a "bean-counter" looks at your case and decides how much they will pay for and what they won't pay for.
But in one case it's "rationing" and in the other - not.
When you're talking about medicaid and medicare, you're not paying for any coverage. Someone else is paying for you and their willingness to provide you all you can eat medical care is zero.
not true.
Your FICA tax pays for Medicare Part A and Part B has premiums. Even Medicaid requires some payment depending on your income.
In ALL countries with UHC AND for ObamaCare - the basic plan is NOT for others to pay for you but for YOU to pay payroll taxes that go into a fund to pay for your care.
The individual mandate requires you to pay for your care - as opposed to not having an individual mandate and taking money from others to pay for your care.
" "they can be denied coverage or denied insurance in the US. That never happens in Canada."
But they are never denied timely treatment. That DOES happen in Canada "
yup but what is worse - denied insurance and access or denied "shorter wait times".
The people without insurance have wait times also - in the ER.
right?
again - you're confusing covering everyone verses not covering everyone.
If you want to get better wait times by insuring only some - but in the end the ones without insurance still get care and is paid for by those who do get insurance - and at the end of the day - such a system ends up with twice the costs per person - is it really a better system?
"friendly amendment - immutable theory not often found in a pure form in the wild."
Total nonsense.
"What you are arguing is for health care costs to go up in order to assure supply."
Again you demonstrate that you have no understanding of supply and demand.
Oh I understand it perfectly well. I go one step further than you and recognize it often does not work in practice the way the theory claims.
It's totally off the wall to claim that in a system that has the highest health care costs in the world - that the problem is not enough "supply".
Healthcare costs are what they are.
really? twice as high as other countries?
"You don't make them lower by not paying the full cost. Price controls don't work, Larry, You will get shortages, rationing, and poor service."
so that's why MRIs cost less than 1/2 overseas than here?
There is no way around it. It's an immutable law
the theory is immutable. Once it gets into practice there are all kinds of things that distort it.
there may well be some things that are bought/sold on a pure supply/demand basis but there are many, many things that are not pure supply/demand markets.
" No, you dim bulb. I'm pointing out that price controls don't work. You can't lower prices by refusing to pay the full cost. "Holding the line" on Medicare payments won't lower the cost of doctor visits. "
you've argued that holding the price down restricts supply - right?
and you've argued that if you take Medicare (price restrictions) out of the loop - prices will rise and assure a better supply, correct?
you're arguing this for a health care system that is already the most expensive in the world and is said to be "better" than the other 35 countries with govt controls on everything.
larry g:"Oh I understand it perfectly well. I go one step further than you and recognize it often does not work in practice the way the theory claims."
Perhaps you don't understand supply and demand as well as you think you do. There's a reason these principles are referred to as "Laws" of supply and demand.
I think I've been as respectful of your comments as anyone, Larry. So consider that when I suggest to you: Please stop wasting everyone's time by trying to argue that you are smarter than the entire economics profession.
It's "laws" of supply and demand, not "theories".
really? is this why Canadians pay extra for American care?
This the only sentence of your brainless drooling I accidentally read as I scrolled down to Jet's post. You are a total moron.
@Jet - I DO appreciate the polite nature of your comments.
re: supply/demand
If one is a pragmatic person, he does not insist that supply/demand works exactly as suggested by the law (I still say theory).
He recognizes that most "markets" are NOT pure, unfettered supply/demand markets and he understands why and he further understand what really happens when markets are distorted.
Those who continue to insist that supply/demand always works as the "law" suggests are disconnected from the realities IMHO.
I do not think I am "smarter" at all but I do think being pragmatic and acknowledging realities is better than insisting something that is not the reality - because you cannot let go of the ideology.
I actually DO believe that we want and should have a more legitimate supply/demand market in HC but we will not get there as long as people continue to insist that the law is "immutable" when obviously our system is totally corrupted as a pure supply/demand market.
the real question is what can you do to make it MORE like a legitimate supply/demand market.
Virtually everyone who posts here acknowledges that we do not have a pure supply/demand market in HC no matter how "immutable" the law is.
My view is that "immutable" does not describe the realities.
we have to recognize that we do not have a pure supply/demand market and why - if we want to reform it.
really? is this why Canadians pay extra for American care?
This the only sentence of your brainless drooling I accidentally read as I scrolled down to Jet's post. You are a total moron.
and Methinks you're a total butt face.
Jet,
From what I've read and written myself, Larry has been made aware of what supply and demand is at least 100 times on this blog. He has been made aware of the fact that not all costs are monetary. Ad nauseam. Had I not encountered Muirdiot at Cafe Hayek, I wouldn't have known people that stupid could survive early childhood.
More importantly, I don't know that there is an answer for an ideal number of physicians. I think that depends on a lot of factors. If you can go to Walmart for a cholesterol check, then maybe you need fewer. If Nurse Practitioners were permitted to do some of the things doctors do, then maybe we need fewer. If the population is healthier, you need fewer.
But, we do know that in Obamacare physicians are the gatekeepers. We also know that lowering the out of pocket cost will increase demand for their services. You need referrals to see anyone else. There are definitely not enough physicians for that and Obamacare is going to make the shortage worse. My physician is the only one of my doctors who still accepts insurance and he thinks there's significant incentive for him to dump insurance altogether. Of course, he's an excellent doctor who is in demand. Lesser doctors probably can't amass a cash-paying clientele. I predict that Obamacare will worsen the shortage of physicians and the available physicians will be mediocre to horrible. The good physicians will either stop taking insurance, get out of the business entirely, or not go into it in the first place (if the rules change, forcing them to take insurance as a condition of licensing - and force is the way I think the U.S. government will handle it). We'll see what happens. They're busy writing the details of what they'll inflict on us right now.
" From what I've read and written myself, Larry has been made aware of what supply and demand is at least 100 times on this blog. He has been made aware of the fact that not all costs are monetary. Ad nauseam. Had I not encountered Muirdiot at Cafe Hayek, I wouldn't have known people that stupid could survive early childhood"
Actually what is REALLY stupid is to INSIST that some "law" is "immutable" when the entire world around you is full of examples of distorted markets that do not operate per the law.
that's what's stupid - Ms. Moron.
Jet & Morganovich,
I just ran into this about heritability of the IQ on the Rational Optimist Blog:
http://www.rationaloptimist.com/blog/iq-heritability-is-testament-to-environmental-equality.aspx
Thanks, methinks, for the link. Ridley's essay is pretty consistent with my understanding: that IQ is inheritable, but that a few environmental factors can inhibit intellectual development. As Ridley states:
"Raise a child hungry or diseased and environment does indeed affect IQ."
Larry G: "Actually what is REALLY stupid is to INSIST that some "law" is "immutable" when the entire world around you is full of examples of distorted markets that do not operate per the law."
Larry, economists have explained those distortions within the framework of the supply and demand laws. A number of factors can shift or alter the slope of demand and supply curves. Taxes, subsidies, regulatory barriers to entry, changes in supply or prices of complimentary and substitute goods are examples. But the impact of all those distortions can still be explained using the supply-demand framework.
Accepting the laws of supply and demand is not a question of being theoretical vs pragmatic. rather, it's a question of whether one is educated in economics or not.
@Jet
I REALLY DO appreciate the civil way you have responded. Thank you.
"Larry, economists have explained those distortions within the framework of the supply and demand laws. A number of factors can shift or alter the slope of demand and supply curves. Taxes, subsidies, regulatory barriers to entry, changes in supply or prices of complimentary and substitute goods are examples. But the impact of all those distortions can still be explained using the supply-demand framework."
Totally Agree. That's why I focus not on the theory but on the way it really is working and what changes might be made to get it back to a system that better operates according to supply/demand.
"getting the govt out of it" is for me a non sequitur. as long as you have a govt, there is going to be distortion.
The question in my mind is can the govt put together a framework that will provide a market that does operate according to supply/demand.
Some people think Singapore has. If you look at what Singapore actually did, there is an argument in favor of that.
Accepting the laws of supply and demand is not a question of being theoretical vs pragmatic. rather, it's a question of whether one is educated in economics or not.
I totally accept the theory/law but I do not believe the real world operates strictly according to that law and I do not believe it is possible for govt to step back so far as to have markets that are completely unfettered and operate totally according to the law/theory.
Just not going to happen in my view.
So I shoot for what I believe is possible.
that's it in a nutshell.
I just don't think advocating for the govt to get out of HC is a reasonable or realistic approach.
I like the give and take of discussing it and I do LEARN from others but I don't buy dogma... and I intensely dislike Ad Hominems and pejoratives in case you have not noticed.
I respond politely to those that do the same.
I won't tolerate the name-callers, it only emboldens them.
Jet, wanna blow his last firing brain cell with giffen goods?
I'm curious, Larry, do you also hold the view that airplanes driving around in the sky indicate that gravity doesn't always work as the theory suggests?
more asinine crap?
Do you have a clue guy that gravity is not the same - not a constant - if full of anomalies that do affect flight and accuracy of ballistic and cruise missiles?
I'm fully cognizant of "theories".
you have to accommodate the fact that theories often do not describe what actually happens.
Here's the reality: " A perfect sphere of spherically uniform density (density varies solely with distance from centre) would produce a gravitational field of uniform magnitude at all points on its surface, always pointing directly towards the sphere's centre. However, the Earth deviates slightly from this ideal, and there are consequently slight deviations in both the magnitude and direction of gravity across its surface. Furthermore, the net force exerted on an object due to the Earth, called "effective gravity" or "apparent gravity", varies due to the presence of other factors, such as inertial response to the Earth's rotation."
so tell me what does the "theory" tell you about gravity?
another example:
" It has been suggested that a number of other goods might be Giffen. While the arguments are theoretically sound (i.e., they accord with Marshall's basic intuition), in each case the supporting empirical evidence has been found to be unconvincing."
so you tell me. Do you use this theory to explain how supply/demand works in an economy or do you look at it as a theory and not necessarily a description of the actual reality?
And I think we now have Larry's answer to Captain profits question: Yes.
Thank you, Captain Profit.
We also know that Larry can google as well as cut and paste. Well done, Larry! But it's all stuff Larry can't understand and there's no evidence that an attempt to understand was even made. Awe....
Let's blow whatever lives between his ears with the concept of elasticity and see what he comes back with.
I do find it interesting that my housekeeper, who has never set foot into a classroom of any kind, has no problem understanding supply and demand, yet Larry struggles.
what Larry Struggles with is you fools who insist on doctrinaire drool to satisfy Libertarian ideological idiocy.
Anyone who thinks supply/demand describes our health care system just is disconnected from reality.
and then they compound it by insisting that it must conform to theory no matter the thousands of distortions that so totally alter it as to render any theoretical explanation as close to ludicrous.
It's not about supply/demand "theory".
except to those whose thinking is so doctrinaire as to separate themselves from any hope of actual changes.
just listening to some of your "solutions" to HC is like listening to loony tunes...
how many elected officials represent your views?
how many countries run the way you think they should?
how about almost none?
how would you change a system politically with your totally off the wall "ideas"?
so this is Alice in Wunderland with some of you guys and name-calling those he point out just how idiotic your thinking is.
you might as well be in a padded room for all the sense you make in terms of the real world.
theories are not the reality. theories will never be the reality.
theories can help you understand why and how a system gets distorted but theories won't help you fix if you insist on theoretical purity.
Your idea of a "good" health care plan exists no where in the world.
Not even close.
and yet you pontificate as if you are actually intelligent enough to form a policy that would work.
No elected official represents your views. Zip. No President. No candidate for President. No member of either House of Congress. No member of the SCOTUS. No Governor. No State Legislature...
doesn't that tell you something about the validity of your "ideas" and "theories"?
re: 3 options
yup.
and it comes with return fire!
I'm game as long as you are!
go for it.
Shit. I think we broke him.
no such luck Lady Loon...
dance around some more, it's entertaining!
:-)
"really? is this why Canadians pay extra for American care?"
Yes, that's exactly why. They can't get the care they need in their own country.
"you've argued that holding the price down restricts supply - right?"
Reducing the amount you are willing to pay reduces the number of doctors who will agree to treat you at that price.
For people dependent on Medicare, "holding the line" reduces the supply of doctors who are willing to treat Medicare patients.
Why is this so difficult for you?
This is the very essence of the law of supply and demand.
Methinks
"This the only sentence of your brainless drooling I accidentally read as I scrolled down to Jet's post. You are a total moron."
Larry has been typing without using the shift key, hoping he will be mistake for morganovich, but by the third word of any sentence it's obvious which of them wrote it.
"The question in my mind is can the govt put together a framework that will provide a market that does operate according to supply/demand."
That's a really easy question, although it may not be so in your mind.
Jet sez: ""Larry, economists have explained those distortions within the framework of the supply and demand laws. A number of factors can shift or alter the slope of demand and supply curves. Taxes, subsidies, regulatory barriers to entry, changes in supply or prices of complimentary and substitute goods are examples. But the impact of all those distortions can still be explained using the supply-demand framework."
Larry sez: "Totally Agree. That's why I focus not on the theory but on the way it really is working and what changes might be made to get it back to a system that better operates according to supply/demand."
LOL
If you *totally agree* why did you go on to disagree?
Perhaps you *totally agree* because you don't really understand Jet's comment.
Here's the reality: " A perfect sphere of spherically uniform density (density varies solely with distance from centre) would...blah, blah, blah.
Now that is *really* impressive, Larry. You know how to copy and paste Wikipedia information into blog comments.
How funny!
Have you found someone to explain to you what the words mean?
What that tells us about the law of gravity is this:
Scientists have explained those distortions within the framework of the universal law of gravitation. A number of factors can shift or alter the force of gravity even at different places on the Earths surface. Distance from Earths center, Relative mass of crustal material, and even inertial response to Earth's rotation. But the impact of all those distortions can still be explained within the framework of the universal law of gravitation.
It's the same with the laws of supply and demand, as Jet pointed out.
Nice work with Wikipedia Larry.
Everyone is immensely impressed, but you didn't answer Captain Profit's question. Did you understand it?
"It has been suggested that a number of other goods might be Giffen. While the arguments are theoretically sound (i.e., they accord with Marshall's basic intuition), in each case the supporting empirical evidence has been found to be unconvincing."
Yeah, yeah, enough already! That wasn't an invitation to show more examples of your incredible Google skill.
Did you understand that second one?
Methinks
"I do find it interesting that my housekeeper, who has never set foot into a classroom of any kind, has no problem understanding supply and demand, yet Larry struggles."
That supports my belief that what we call education is over-rated.
(You may want to turn your volume down)
Hey! -- Teacher! -- Leave us kids alone!
Post a Comment
<< Home